Lauren Ritterhouse, MD, PhD
Associate Director, Center for Integrated Diagnostics
Massachusetts General Hospital
Assistant Professor, Pathology, Harvard Medical School

Ibiayi Dagogo-Jack, MD
Thoracis Oncologist, Massachusetts General Hospital
Assistant Professor of Medicine, Harvard Medical School
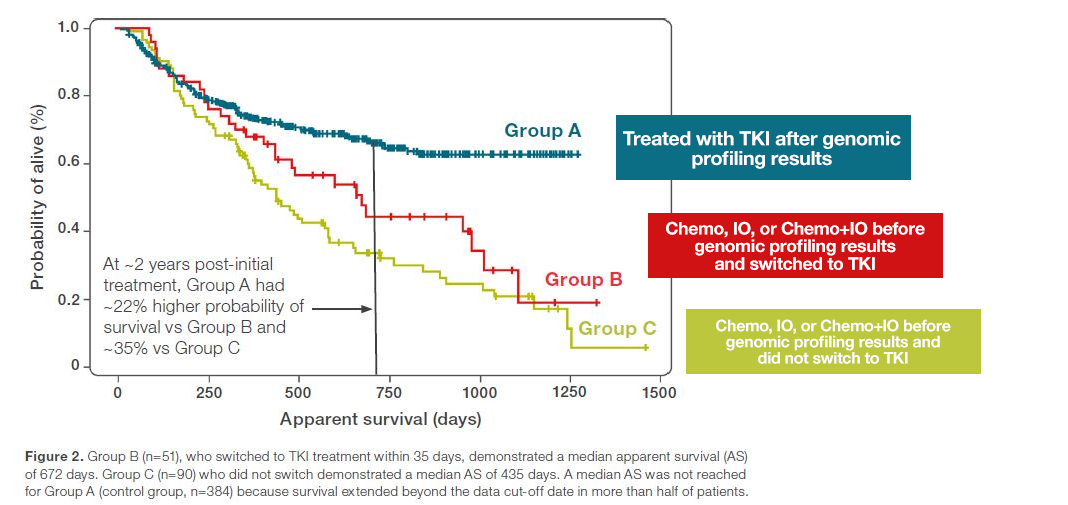
Targeted, cancer genomic profile guided cancer therapy is improving patients outcomes, as was shown among others in the IntegraConnect Study. Patients treated in first line based on their genomic profile have 22% higher probability of survival two years from diagnosis1.
As number of biomarkers associated with targeted treatments keeps increasing, there is more hope for cancer patients. It is expected to be 21 just in NSCLC already in 20252.

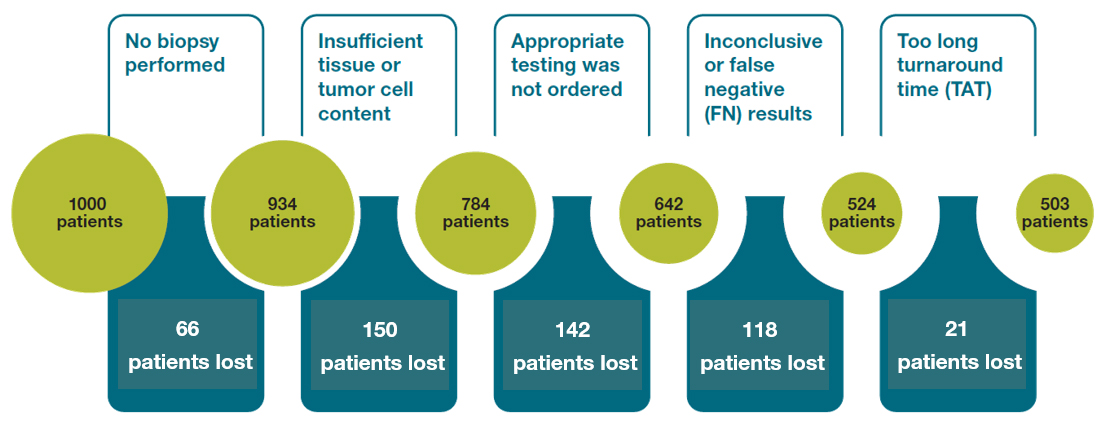
But there are still gaps in a process of providing oncologists with the genomic profile data in time. These gaps are hindering patients access to the treatments they could potentially benefit from1,3.
Based on the published data and experience from many leading cancer centers, there is emerging a solution -
“Rapid Lung NGS”:

Lauren L. Ritterhouse, MD, PhD
Massachusetts General Hospital Department of Pathology and Center
for Integrated Diagnostics
"With our rapid-lung NGS program and > 95% sequencing success rate we strive to provide our oncology colleagues with all of the clinically recommended biomarkers in the first-line setting available to them when making therapy decisions."
On-Demand Webinars
In this free, on‑demand webinar, Dr. Brandon Sheffield of Canada‑based William Osler Health System shares the organization's experience with implementing next‑generation sequencing (NGS) in routine oncology biomarker testing.
In their pilot study, 578 solid tumor samples underwent genomic profiling. All testing was performed by one group of technologists within the same division of the laboratory, achieving a median turn‑around time (TAT) of three business days.


Dr. Brandon Sheffield, MD
Medical Director, Advanced Diagnostics
Physician Lead of Research
Department of Laboratory Medicine
William Osler Health System
Democratization of NGS is the key to accelerating cancer care.

![]()
"Significantly shorter time to results enables faster and optimal treatment decisions."
![]()
"It improves care coordination between multidisciplinary teams, leading to true personalized medicine."
![]()
"Small sample requirement provides biopsy stewardship,
“tissue saving”."
![]()
"Allows for the development of local expertise in biomarker testing to support the future of precision medicine."
Have questions? We look forward to speaking with you about bringing NGS to your lab.

Subscribe here to stay abreast of the latest news about NGS in precision oncology.