
Dr. Bekim Sadokovic
Western University
Quote taken from:
Eur J Haematol. 2019 Sep;103(3):178-189.
The classic approach to molecular hematology testing involves targeted single-analyte testing after initial pre-screening by other diagnostic modalities including flow cytometry, anatomic pathology, and clinical cytogenetics. This approach presents several limitations:
WGS identifies every DNA base across the entire genome (coding, noncoding, mtDNA) and detects all variant types (SNVs, Indels, SVs, CNVs).19 With its massive data set, WGS entails substantial costs, extended time to results (weeks), and complex data interpretation, making it a method better suited for research and discovery rather than routine clinical testing.3,19
Targeting the protein-coding regions of the genome, WES detects coding variants (SNVs, indels).19 Due to the cost, length of time to results (weeks), and the complexity of data interpretation, WES is better suited for research and discovery than routine clinical testing.3,19

WTS identifies genome-wide differential RNA expression (coding and noncoding). By evaluating altered genetic variants and the continuously changing cellular transcriptome, WTS provides valuable information about the cells and transcriptional networks.20 It is commonly used for discovery and gene-expression analysis.20

Targeted-sequencing panels profile a select set of genes that are curated for a specific application or disease.20 Featuring actionable biomarkers and a smaller data set, these panels are commonly used in clinical applications to help inform the diagnosis, treatment, and monitoring of individual patient disease states.3
When it comes to acute hematological malignancies, early diagnosis and personalized disease management present substantial challenges, as does the reliable and timely detection of measurable residual disease (MRD) —essential to guiding therapy choices, monitoring treatment response, and detecting relapse.3 Genomic biomarkers are the key to unlocking this valuable clinical information.1,3,15
While the value of WGS and WES in studying hematological malignancies is recognized, applying these methods for routine clinical testing is impractical due to costs, long turnaround time to results (weeks), and the complexities of data storage, analysis, and interpretation.3
With their actionable biomarkers, quick turnaround times, and lower cost compared to WES, targeted NGS gene panels are best suited for routine clinical applications and especially ideal for identifying mutations and translocations in specific genes.1,3,16 Some advanced NGS platforms deliver robust integrated analysis and reporting tools, empowering clinicians to facilitate patient selection and clinical trial inclusion.12,21
Relying on the high sensitivity of NGS, clinicians can utilize it to monitor multiple mutations over time to better track a patient’s evolving mutational landscape.9,15 NGS promises to advance precision medicine by identifying actionable biomarkers and individual disease mutations and matching patients to clinical trials, all ultimately contributing to the development of novel, targeted therapies, tailored disease management, and better outcomes.1,3,12,21


Dr. Kojo Elenitoba-Johnson, MD
Peter C. Nowell, M.D. Professor of Pathology and Laboratory Medicine
Perelman School of Medicine at the University of Pennsylvania
Director, Center for Personalized Diagnostics
Director, Division of Precision and Computational Diagnostics
Rapid assessment of genetic biomarkers in myeloid malignancies is vital for early diagnosis, first-line therapy choices, and ongoing clinical disease management.3,29 This includes evaluation of therapy response and relapse/measurable residual disease (MRD) detection.3,29 In particular, acute diseases like AML require rapid test results for key diagnostic and risk stratification markers (ie, PML-RARA gene fusion, FLT3 or IDH1/2, and NPM1).3,15 The 2017 ELN guidelines recommend that results for FLT3 and NPM1 be available within 72 hours.15
"There are several protocols, including extensive amounts of genetics and immunophenotyping, which are required to establish the appropriate approach to treat patients. The sooner we can get results and deliver treatment, the better the outcomes."
Advances in AML risk-stratification guidelines and targeted therapies have made it increasingly important for clinicians to consider a wide range of genetic biomarkers to guide front-line patient-care decisions.3,15,29 NGS helps to address this need by rapidly providing results for a broad number of genetic targets.3 The latest instruments enable a laboratory to sequence a patient sample in about 24 hours so clinicians can have the results in days.3

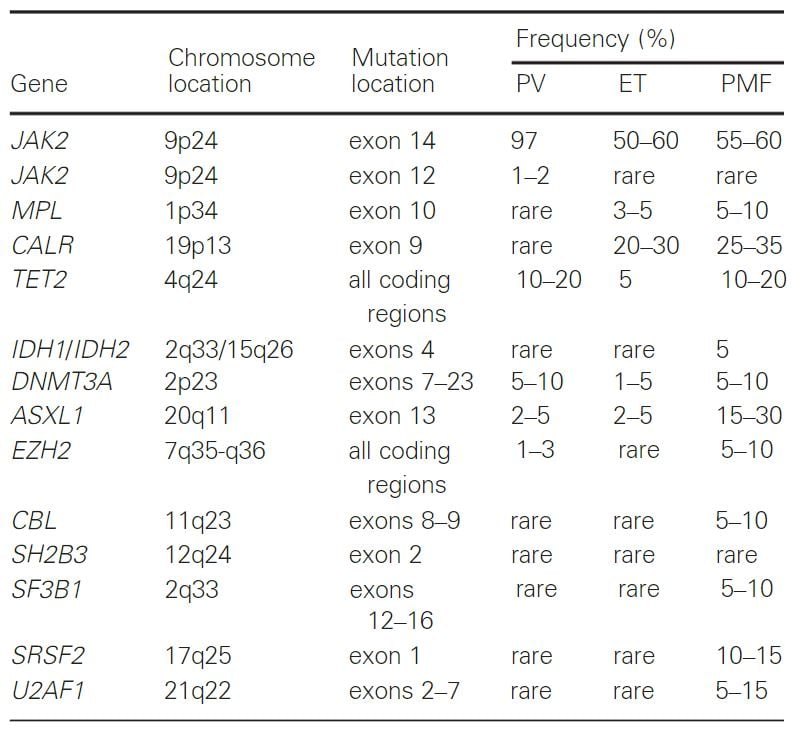
PV, polycythemia vera; ET, essential thrombocythemia; PMF, primarymyelofibrosis
Detecting leukemic drivers with NGS informs disease management
Over the last decade, NGS has helped unravel the complex molecular underpinnings of myelodysplastic syndromes (MDS).35 Dozens of recurrent mutations associated with the disease have been revealed.35 Targeted sequencing will typically identify at least 1 mutation in the majority of cases.35 While NGS does not replace conventional cytology, histology, and cytogenetics, it can provide meaningful insights from diagnosis and prognosis to treatment response in MDS patients.35
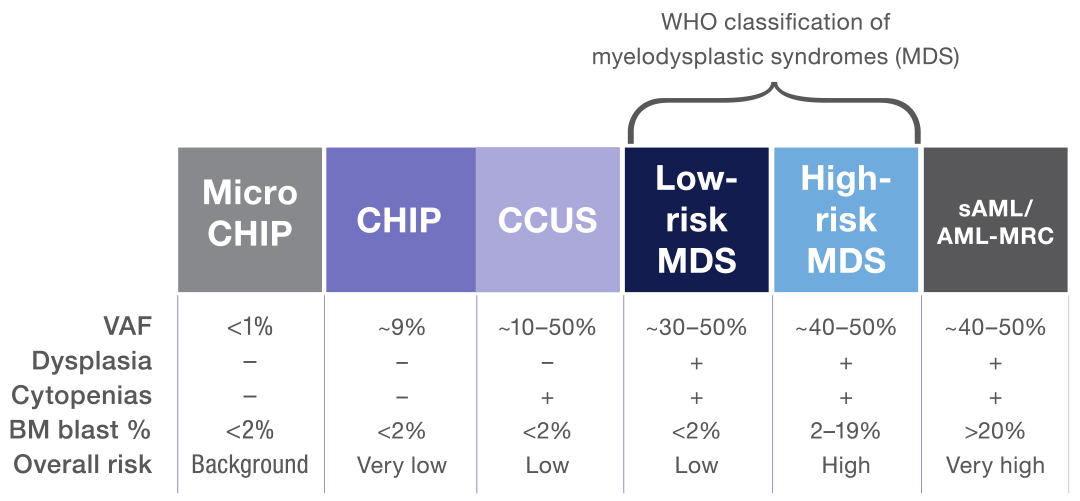
MDS is a clonal disease arising from the proliferation of mutated hematopoietic stem cells.12,35 The spectrum of clonal myeloid disorders ranges from clonal hematopoiesis of indeterminate potential (CHIP) to secondary acute myeloid leukemia (sAML).35,38 MDS is characterized by peripheral blood cytopenia, dysplasia, and the absence of features that define acute leukemia.12,38 In cases where clonal hematopoiesis is detected in the absence of a cytopenia or dysplasia, mutational data can help distinguish MDS from CHIP.38 Typically, a larger number of mutations with a higher variant allelic frequency (VAF) are more supportive of an MDS diagnosis.38
Notably, mutational data of clonal myeloid disorders can also help inform the level of risk for a particular disease to progress to another more serious disorder (eg, clonal cytopenia of undetermined significance [CCUS] evolving to MDS and MDS evolving to sAML).12,38,39
Ongoing research in this area is likely to increase the clinical relevance of NGS for diagnosing and treating these disorders.12,21,35
Since the 1970s, the standard of care for AML has been cytotoxic chemotherapy, and long-term overall survival has remained relatively poor.40 Progress in the development of mutation-targeted therapies in recent years is transforming the AML treatment paradigm.40 Finally, there are more options for patients, and with them, the promise of better clinical outcomes.40
NGS has helped identify many significant genetic alterations, leading to the development of therapeutics that target specific gene mutations.40 In 2017, midostaurin became the first tyrosine kinase inhibitor (TKI) approved for FLT3-mutated AML; many more targeted therapies are emerging, including the IDH2 inhibitor, enasidenib for relapsed/refractory (R/R) AML.40 While further research is needed to understand all the genomic complexities at play, it is apparent that these new targeted therapies are raising the standard of care for AML and improving overall survival and quality of life.40
With its comprehensive genetic profile of the disease, including targetable mutation and other genetic abnormalities, NGS can offer tremendous clinical insights into AML, from risk stratification and therapy selection to disease monitoring.40

Recurrence monitoring and measurable residual disease (MRD) detection are critical for hematological disorders.1,3,17 While our improved understanding of the molecular landscape of AML has resulted in more informed and targeted first-line treatments, the threat of disease relapse is always looming.40 Studies have shown that negative MRD (assessed by molecular techniques or immunophenotyping) may be a better predictor of survival as it’s associated with a lower risk of relapse.3
Chart: NGS identification of clonal and subclonal mutations in AML provides insights into prognosis, treatment, and response.21
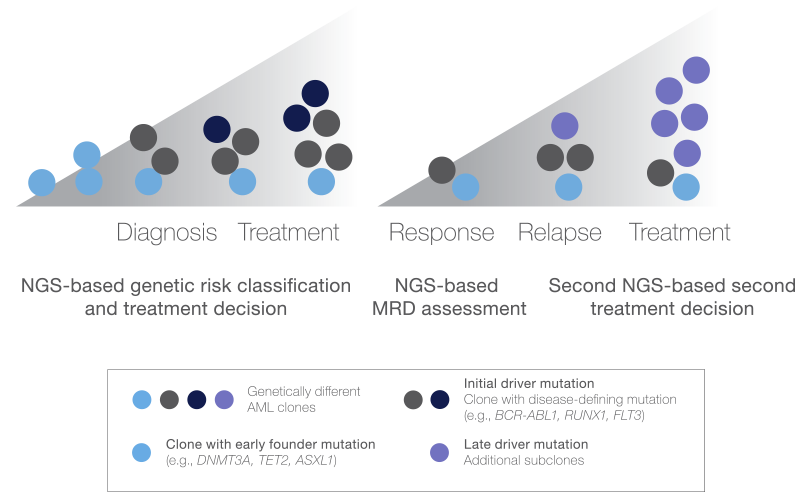
This schematic depicts the subclonal genetic heterogeneity of AML development and progression and illustrates the critical role of NGS in the assessment of clonal and subclonal mutations throughout disease management.
By traditional standards, complete remission is achieved when a morphological assessment shows < 5% myeloblasts (immature myeloid cells) in the bone marrow, absence of circulating blasts, and hematologic recovery.21 Although most AML patients achieve complete remission after primary treatment, many eventually relapse, indicating that morphology is not the best predictor of survival.21
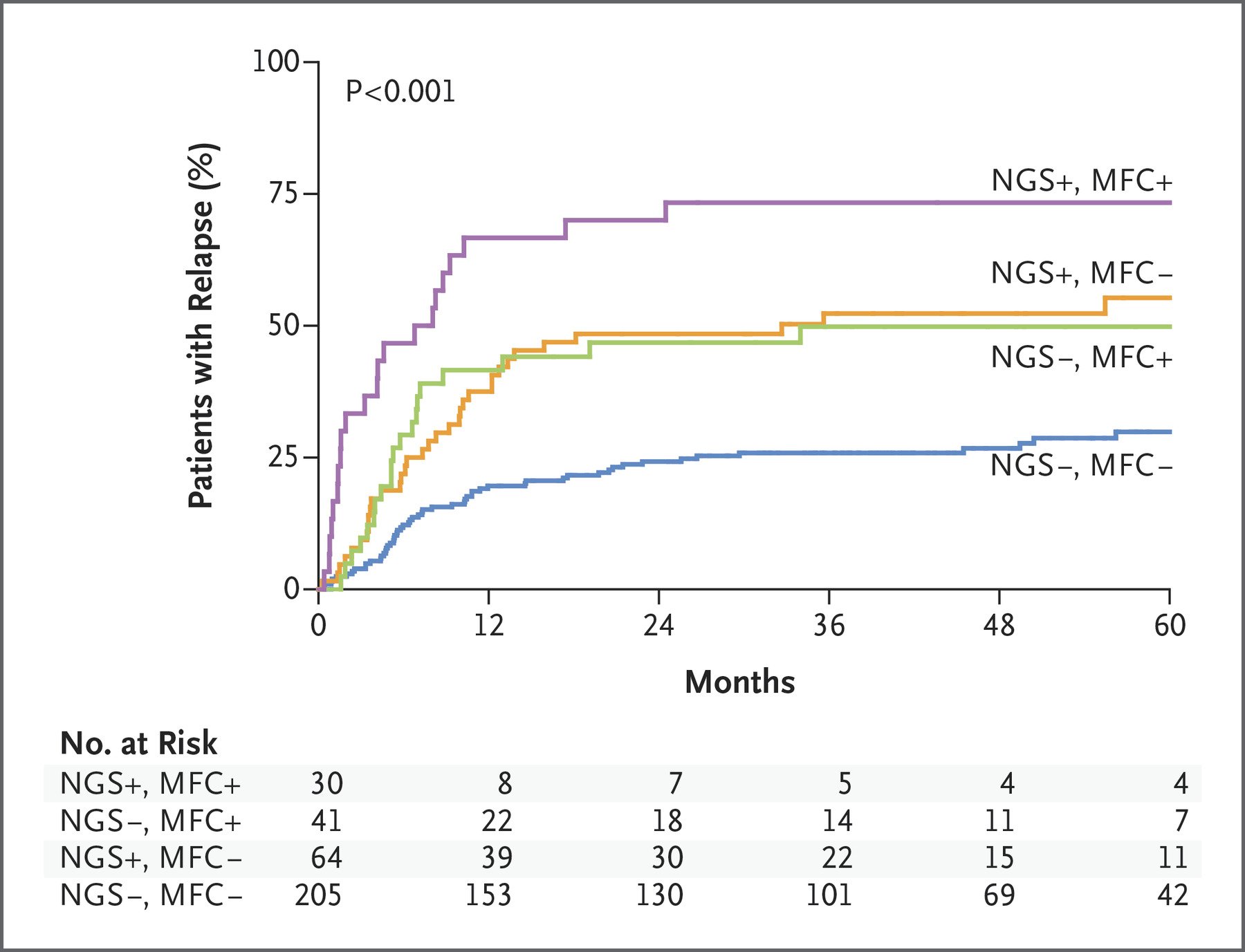
CHART: Studies demonstrate the prognostic value of NGS and multiparameter flow cytometry (MFC) MRD for AML relapse (~75% concordance)41,42 (Source)
Given AML’s combinatorial complexity and mutational combinations (3 to 5 driver mutations in more than 250 genes), NGS offers multiple advantages for MRD.44 NGS can detect the persistence of disease-specific variants to inform treatment and prognosis and identify patients at high risk for early relapse so they can benefit from closer tracking and additional therapies (stem cell transplants).1,3,16, 37,44
Benefits of NGS:

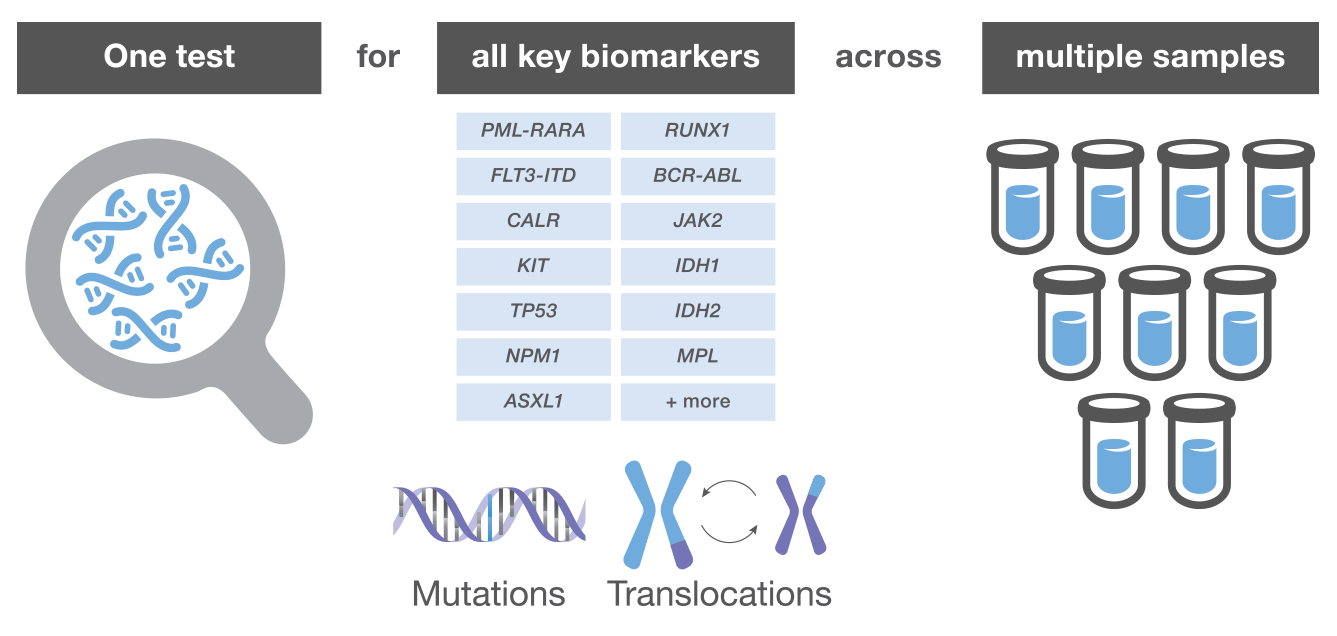
Advances in NGS workflow automation and integrated reporting have empowered clinicians to perform simultaneous assessments of multiple target genes in routine laboratory analysis.1,3,16 An ever-growing list of biomarkers and their inherent genetic complexity have made myeloid malignancies the proving ground for this new testing paradigm.1,2
The value of integrating NGS into daily clinical practice for rapid, streamlined analysis and utility across the care continuum is no longer in question.1,3,15,16,21,29,32 Assessment of myeloid neoplasms with targeted NGS panels is demonstrated to improve diagnosis, assist therapeutic decisions, inform prognosis, and better detect measurable residual disease.1 Adoption of in-house NGS brings advanced molecular diagnosis and precision oncology to more patients and will help raise the standard of care.1-3,12,27,32,40

Historically, cancer treatment was limited to a one-size-fits-all model, where therapies were selected based on the cancer type (site) alone. Today, NGS has advanced the understanding of cancer biology so many therapy decisions can be based on specific cancer biomarkers, and genetic alterations in an individual’s cancer genome.1-3,13,24
Empowered with a molecular profile of a patient’s cancer, clinicians can tailor treatments to optimize outcomes and prescribe therapeutics that directly target biological pathways while avoiding sub-optimal therapies.1-3,13,24
Imagine every oncology patient receiving treatment individualized to their specific cancer genome. What was once a vision for improved cancer care is finally a reality—a world where molecular insights transform clinical care, improve outcomes, and enhance the quality of life for patients.

Speak with a representative about myeloid testing with next generation sequencing for your lab today.