Introduction
While next-generation sequencing (NGS) has enabled molecular characterization of tumors supporting the development of an increasing number of biomarker-driven targeted therapies, access to biomarker testing and ultimately therapies remain suboptimal. The levels of biomarker testing differ greatly across practice settings due to challenges with implementing complex precision oncology programs in the clinical setting [1].
Patient access to biomarker testing relies on a combination of factors. Challenges with bio-specimen collection including insufficient tissue or tumor cell content, turnaround time delays, and test performance can collectively prevent patients from receiving biomarker-informed treatments.
Furthermore, highly specialized testing, such as homologous recombination deficiency testing performed in central laboratories, may be cost prohibitive or simply unavailable in certain countries. Thus, efforts addressing implementation challenges may improve clinical care by making biomarker testing more readily available for the broader population.
What is HRR and HRD?
Our cells are continuously subjected to endogenous and exogenous sources of DNA damage. To support survival and reproduction, maintaining genome stability is critical for all cells. This involves complex networks of proteins and signaling pathways; with multiple mechanisms whose activation depends on the type of DNA damage and when it occurs during cell division.
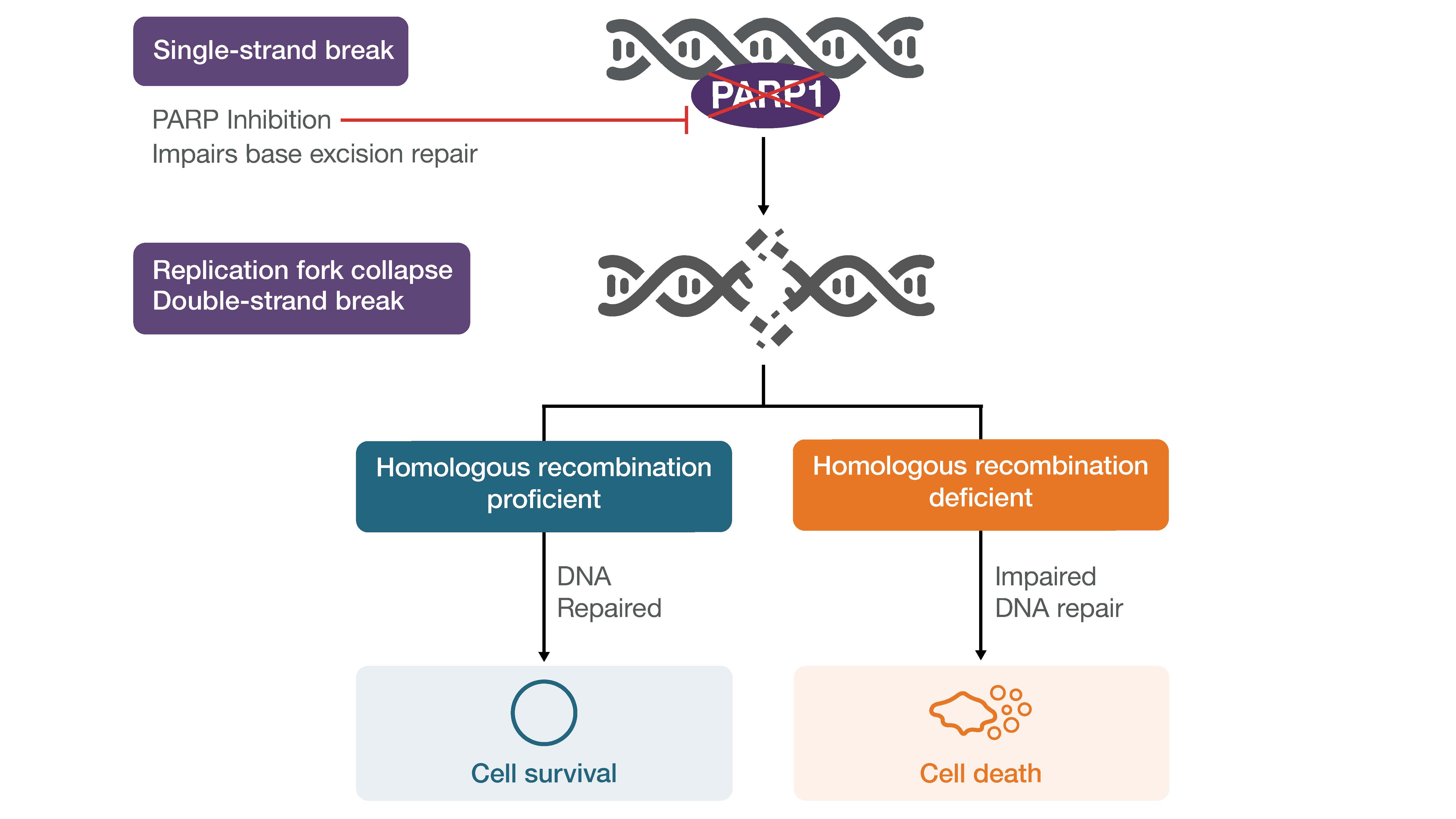
Homologous Recombination Repair (HRR) is a critical pathway that relies on several proteins including BRCA1 and BRCA2 to enable high fidelity repair of double-stranded DNA breaks in a template dependent manner [2].
Homologous Recombination Deficiency (HRD) is the inability to repair double-strand DNA breaks using the HRR pathway, which can be caused by mutations in BRCA1 and BRCA2 as well as other genes involved in the HRR pathway [2]. Cells with non-functioning HRR rely on other lower fidelity error-prone DNA repair pathways that lead to the accumulation of genome wide alterations such as insertions and deletions, copy number alterations, or structural rearrangements, and can be detected by molecular methods as genomic scars.
Why Measure HRR and HRD Status?
The assessment of HRR gene mutations and HRD status has prognostic and predictive value in certain cancer types, supporting the incorporation of molecular testing into patient management.
The understanding of BRCA1 and BRCA2 biology has driven the development of therapeutic approaches that target HRD, namely poly(ADP-ribose) polymerase (PARP) inhibitors via synthetic lethality [2,3].
For example, in ovarian cancer, BRCA1 and BRCA2 mutation status can provide insight into the course of disease and HRD status could be used to guide treatment decisions given the sensitivity of tumor cells to PARP inhibitors and platinum-based chemotherapy.
Therefore, knowledge of BRCA1 and BRCA2 mutation status along with HRD status is crucial for an appropriate management plan for patients.
How to Measure HRD Status?
There are two key approaches for the assessment of HRD status:
1) Detecting mutations in HRR genes, or the “causes” of HRD: Genetic or epigenetic alterations in HRR genes can cause a loss-of-function in the HRR pathway leading to the HRD phenotype in various cancer types. BRCA1 and BRCA2 play prominent roles in the HRR pathway and impaired BRCA gene function is the most studied mechanism that results in HRD. Alterations in other HRR pathways genes have also been associated with the HRD phenotype [2,4].
2) Measuring the “consequence” of HRD though the presence of genomic scarring/instability: The consequence of error-prone DNA repair through alternative pathways is the accumulation of double strand DNA breaks presenting as genomic scars. Assessing and quantifying genomic scars serves as an indirect measure of HRD irrespective of the underlying causes [2,4].
Improving Access to HRD Testing
The U.S. FDA has approved several companion or complementary diagnostics to aid in the selection of patients for the treatment with PARP inhibitors. However, to date, these FDA approved assays are performed in central laboratories [4].
To address the limited accessibility of HRD testing, multiple initiatives are underway globally including the European ENGOT (European Network of Gynecological Oncology Trial) HRD Initiative and The Friends of Cancer Research HRD Harmonization Project [5].
The European ENGOT HRD Initiative is developing new HRD tests based on samples from the phase III PAOLA-1 trial, which randomized patients with advanced ovarian cancer to investigate a PARP inhibitor combination regimen.
The Friends of Cancer Research, in partnership with commercial companies, is currently working Phase 3 of the HRD Harmonization Project, collectively aimed at addressing the lack of consistency around HRD to better identify and care for patients who are most likely to benefit from targeted therapies.
Phase 1 led to a publication in The Oncologist describing opportunities and best practices to align the definition of HRD and the parameters that contribute to the determination of HRD status [2]. Phase 2, presented at the Association of Molecular Pathology 2022 Annual Meeting, compared 11 assays that measure HRD using an in silico ovarian cancer dataset [6].
The analysis demonstrated variability, both in factors used for determining HRD status and the status calls across assays. In the survey of HRD assays, factors beyond BRCA1 and BRCA2 mutation status for the determination of HRD status included:
| HRD assay factors among HRD Harmonization Project participants | |
| HRD Score | TAI inclusion |
| gLOH cutoff | LST inclusion |
| gLOH inclusion | Methylation in non-BRCA HRR pathway genes |
| BRCA1/2 inactivation | Mutations in non-BRCA HRR pathway genes |
Phase 3 of the project is underway and consists of analyzing freshly extracted DNA from formalin-fixed paraffin-embedded ovarian tumor samples. While there is currently no “gold standard” for measuring HRD, this will provide additional context into the variability in assessing HRD status.
Conclusion
It is crucial that HRD testing is harmonized across diverse methodologies in order to realize the potential of PARP inhibitors and maximize benefits for patients with ovarian, and other cancer types.
Current commercially available HRD assays have shortcomings including labor intensive and complex workflows, which may not be feasible for local laboratories performing routine biomarker testing.
Automated and streamlined testing solutions are required so HRD testing can be performed in local laboratories, closer to patients, to help unlock the full potential of precision oncology.
References:
1. Smeltzer MP, et al. The International Association for the Study of Lung Cancer global survey on molecular testing in lung cancer. Journal of Thoracic Oncology 15.9 (2020): 1434-1448.
2. Stewart MD, et al. Homologous recombination deficiency: concepts, definitions, and assays. The Oncologist 27.3 (2022): 167-174.
3. Lord CJ and Ashworth A. PARP inhibitors: the first synthetic lethal targeted therapy. Science (New York, NY) 355.6330 (2017): 1152.
4. Herzog TJ, et al. Testing for homologous recombination repair or homologous recombination deficiency for poly (ADP-ribose) polymerase inhibitors: A current perspective. European Journal of Cancer (2022).
5. The Friends of Cancer Research HRD Harmonization Project ttps://friendsofcancerresearch.org/hrd/ (accessed 1/17/2023)
6. The Friends of Cancer Research HRD Harmonization Project https://friendsofcancerresearch.org/wp-content/uploads/AMP-Poster-FINAL.pdf (accessed 01/17/2023)


A recently published article by the BLOODPAC Consortium details the potential of liquid biopsy in the management of cancer and highlights the barriers to adoption, particularly in underserved populations.
Cancer is one of the leading causes of...
Precision medicine is rapidly changing our understanding of cancer research and treatment decisions. These breakthrough, personalized treatments hold promise even for patients with historically hard-to-treat diseases, like lung or breast cancer. But
Dr. Eric Vail is Director of Molecular Pathology, Cedars-Sinai Medical Center,Los Angeles, California
Can you please introduce yourself and your laboratory?
I'm the director of the Cedar Sinai Medical Center Molecular Pathology Laboratory, which...