Next-generation sequencing (NGS) has become an increasingly important tool for identifying molecular biomarkers that can help guide treatment decisions for cancer patients.
Because of its high level of complexity, NGS testing has traditionally been performed only by specialized academic or commercial laboratories, but NGS is increasingly being implemented locally within hospital pathology labs via advances in automation.
For those healthcare institutions considering the decision to bring NGS in-house, an important question must first be answered: is in-house NGS economically viable?
A new healthcare economic analysis published in the Journal of Health Economics and Outcomes Research indicates the answer could be yes. The potential financial impact of utilizing in-house NGS on hospital budgets was analyzed using two different metastatic non-small cell lung cancer (mNSCLC) testing workflows.
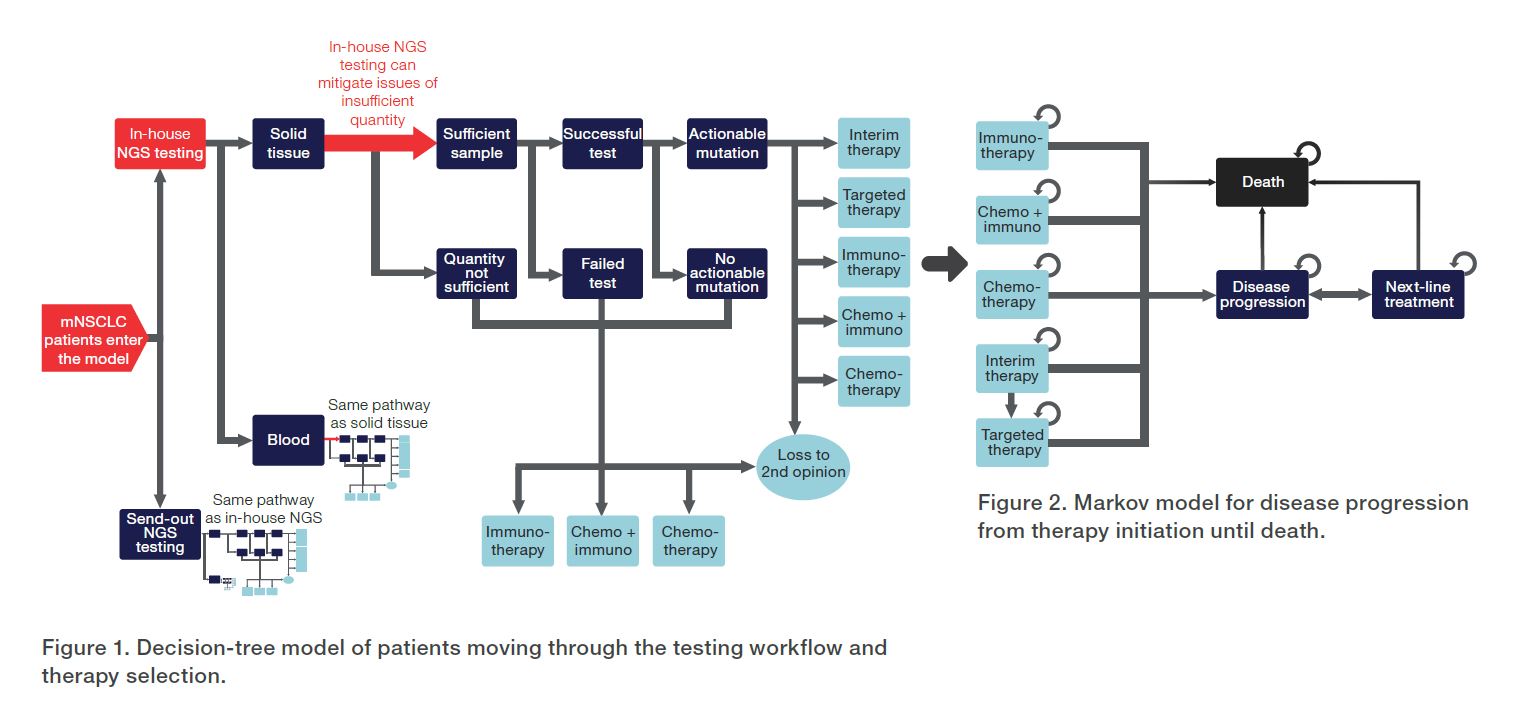
In the first scenario, the hospital would send out 100% of testing to reference labs, while in the second scenario, the hospital would bring 75% of testing in-house and send out only 25% of cases. A decision-tree model was used to simulate movement of patients through the testing pathway (Figure 1), and a Markov model was used to simulate disease progression assessed over 5 years (Figure 2). Key model inputs were derived from a combination of real-world data, peer-reviewed literature, and expert opinions (Table 1).
| Parameter | Value |
| Cost of in-house NGS testing, per test | $600* |
| Cost of sending out NGS testing, per test | $300*† |
| Cost of single-gene testing, per test | $141 [3] |
| Acquisition cost of in-house NGS | $200,000** |
| Reimbursement for in-house NGS testing, per test | $580 [4] |
| Revenue per hospital visit | $124 [5] |
| TAT for sending out NGS testing, in days | 10.3–27.8 [2,6] |
| TAT for in-house testing, in days | 3 [6,7] |
* List price of laboratories.
** Expert opinion.
† $3,000 per test sent out with 10% of invoices funded by hospital ($300).
The resulting analysis revealed that for a US hospital with 500 mNSCLC cases per year, the return on investment (ROI) for bringing 75% of NGS in-house was approximately $1.25 million over 5 years. Although costs increased by $0.71 million in this scenario compared to sending out 100% of testing, revenue increased even greater by $1.73 million.
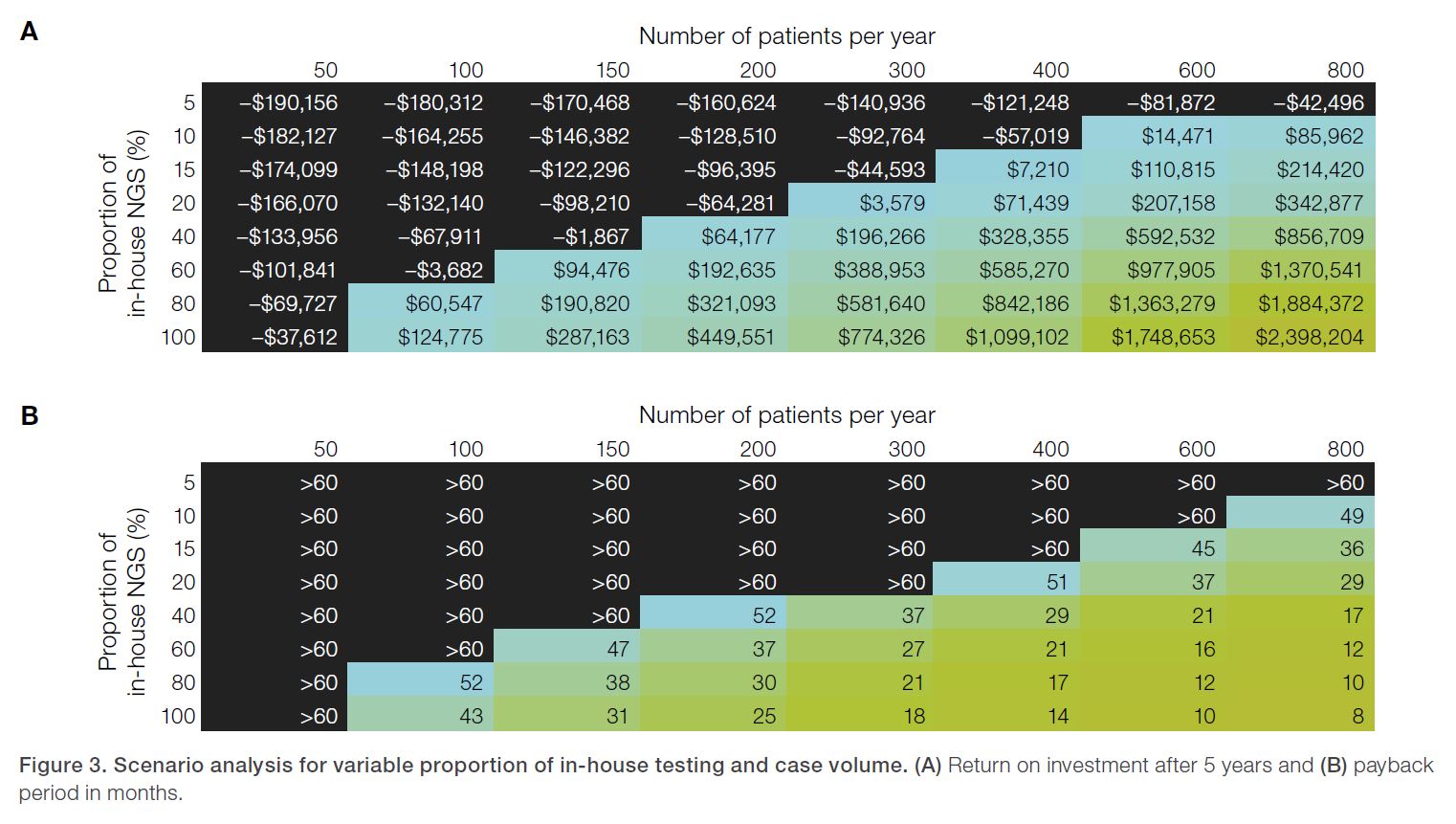
Furthermore, the hospital would break even on the initial investment of 75% in-house testing after only 15 months of implementation [1]. The authors performed an analysis of additional scenarios to evaluate variable patient volume and proportion of in-house testing (Figure 3), finding that more cases would require less in-house testing to break even and vice versa.
For example, a hospital with only 100 cases per year would require 80% or more in-house testing to break even in 5 years, while a hospital with 800 cases per year could break even with only 10% in-house testing. Hospitals with both large case volumes and high proportions of in-house testing would see the greatest return and shortest time to generate a positive ROI [1].
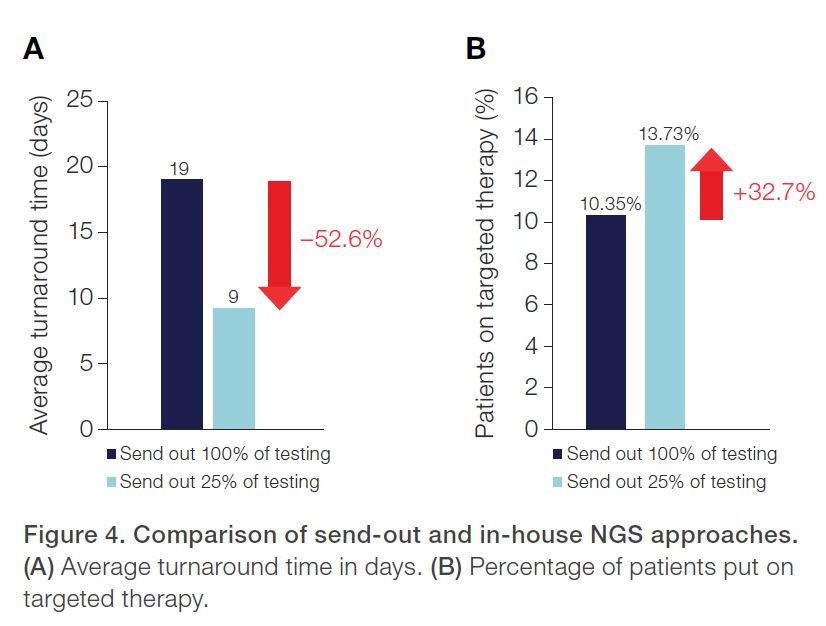
Another observation from the authors was that in-house testing could significantly reduce turnaround time (TAT), leading to an increase in the number of patients put on targeted therapy (Figure 4).
Inclusion of 75% in-house testing reduced average TAT to 9 days, down from 19 days with 100% of testing being sent out, a relative decrease of 52.6% (10 days). In turn, patients treated with targeted therapy rose to 13.73% with inclusion of 75% in-house testing, up from 10.35% with all cases being sent out, a relative increase of 32.7% (3.38% overall) [1].
Separate analysis from another study has shown a high correlation between increased utilization of targeted therapy and increased survival in advanced NSCLC patients [8]. Lastly, because of the increased availability of testing results and associated targeted therapies, the move to 75% in-house testing resulted in 63% fewer patients lost to second opinion (64 patients versus 173 patients in the 100% send-out scenario) [1].
A hospital with 500 mNSCLC cases per year could potentially achieve an ROI of $1.25 million over 5 years with in-house NGS.
Going back to the initial question posed at the beginning of this technical note—is in-house NGS testing economically viable?
This recent healthcare economic analysis implies the answer is yes. Even for hospitals with only 100 cases per year, in-house NGS testing appears to be within reach, and a positive return on investment could be achieved in less than 5 years.
For institutions with higher testing volumes, or those willing to take on a higher proportion of in-house testing, the economic case may be even stronger. Because of advances in automation, NGS is more accessible than ever, and in-house testing for cancer patients could prove to be a savvy financial decision for healthcare institutions.
References
1. Silas U, et al. Fast in-house next-generation sequencing in the diagnosis of
metastatic non-small cell lung cancer: a hospital budget impact analysis. JHEOR. 2023:10(1):111-118.
2. Smith R, et al. (2021) Retrospective analysis using real-world data (RWD) in
predominantly newly diagnosed stage 4 non-small cell lung carcinoma (NSCLC-4) to determine the effect of genomic profiling on treatment decisions. Journal of Molecular Diagnostics 23(11):1632.
3. Johnston KM, Sheffield BS, Yip S, Lakzadeh P, Qian C, Nam J. Costs of in-house genomic profiling and implications for economic evaluation: a case example of non-small cell lung cancer (NSCLC). J Med Econ. 2020;23(10):1123-1129. doi:10.1080/13696998.2020.1789152.
4. Sabatini LM, Mathews C, Ptak D, et al. Genomic sequencing procedure microcosting analysis and health economic cost-impact analysis: a report of the Association for Molecular Pathology. J Mol Diagn. 2016;18(3):319-328. doi:10.1016/j. jmoldx.2015.11.010.
5. Vanderpoel J, Stevens AL, Emond B, et al. Total cost of testing for genomic alterations associated with next-generation sequencing versus polymerase chain reaction testing strategies among patients with metastatic non-small cell lung cancer. J Med Econ. 2022;25(1):457-468. doi:10.1080/13696998.2022.2053403.
6. Sheffield BS, Beharry A, Diep J, et al. Point of care molecular testing: communitybased rapid next-generation sequencing to support cancer care. Curr Oncol. 2022;29(3):1326-1334. Published 2022 Feb 23. doi:10.3390/curroncol29030113.
7. Ilié M, Hofman V, Bontoux C, et al. Setting up an ultra-fast next-generation sequencing approach as reflex testing at diagnosis of non-squamous non-small cell lung cancer; experience of a single center (LPCE, Nice, France). Cancers (Basel). 2022;14(9):2258. Published 2022 Apr 30. doi:10.3390/cancers14092258.
8. Smith R, et al. Evaluation of outcomes in patients (pts) with stage 4 non-small cell lung cancer (NSCLC 4) harboring actionable oncogenic drivers (AOD) when treated prior to report of mutation without tyrosine kinase inhibitors (TKI): an Integra Connect Database (ICD) retrospective observational study. Journal of Clinical Oncology. 2022;40(16):1530. doi: 10.1200/JCO.2022.40.16_suppl.1530.
Thermo Fisher Scientific has provided this resource in order to help the recipient understand the benefits of in-house NGS testing. All information has been provided for informational purposes only. Thermo Fisher Scientific makes no express or implied statement, promise or guarantee related to: (1) The propriety of seeking reimbursement for any item or utilizing a particular code or service;
(2) A payer organization’s decision whether to reimburse; (3) Any level of reimbursement, payment, or charge; or (4) The accuracy of the information included herein. The resource is not intended to increase or maximize reimbursement by any payer. It is the responsibility of the recipient to: (a) Obtain current, accurate information from government payers and commercial payers; and (b) Identify and learn more about local and/or payer-specific reimbursement policies and practices.


How can we enhance the clinical utility and accessibility of liquid biopsy NGS?
Liquid biopsy next-generation sequencing (NGS) holds great promise in therapy selection for oncology, offering non-invasive and real-time insights into tumor genetics,”...
Introduction
In a recent interview with the Anatomical and Molecular Pathology Lab at Sydpath, St. Vincent Hospital, Senior Staff Specialist Dr. Tao Yang and Senior Hospital ScientistDr. Bin Wang shared valuable insights into the significant...
Recently, Thermo Fisher Scientific sat down with Carolina Felix, Senior Biomedical Scientist at the Liverpool Clinical Laboratories (LCL) Molecular Pathology Service, to learn about her lab’s experience working with Thermo Fisher’s Service and...